Overview
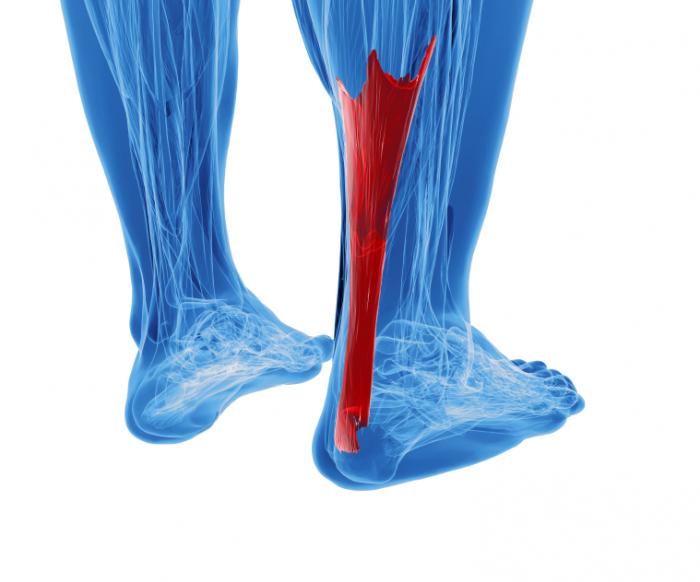 A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture.
Symptoms
Following are a few of the symptoms usually associated with an Achilles tendon rupture. Sudden, severe pain, swelling, bruising, difficulty walking. Sometimes a gap may be felt in the tendon. The most common ways an Achilles tendon rupture is diagnosed are clinical history (presenting symptoms). Thompson or Simmonds test, positive if when squeezing the calf there is no foot movement (passive planter flextion). OBriens test, needles are placed into the tendon; tendon is intact if when the foot is moved up and down, the needle hub moves in the same direction as the toes (opposite direction of the tendon) Ultrasound and MRI, because these technologies involve an added expense, they are usually employed only to confirm the diagnosis.
Diagnosis
A typical history as detailed above together with positive clinical examination usually will clinch the diagnosis. In an acute rupture, one can usually feel the gap in the tendon from the rupture. There may be swelling or bruising around the ankle and foot of the injured leg. With the patient lying on the tummy (prone position) with the knee flexed, the examiner should see the ankle and foot flex downwards (plantarward) when squeezing the calf muscles. If there is no movement in the ankle and foot on squeezing the calf muscle, this implies that the calf muscle is no longer attached to the heel bone due to a complete Achilles tendon rupture.
Non Surgical Treatment
The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex, Advil, Motrin, Naprosyn. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.
Surgical Treatment
Surgery is a common treatment for a complete rupture of the Achilles tendon. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons. Surgical complications can include infection and nerve damage. Infection rates are reduced in surgeries that employ smaller incisions. After treatment, whether surgical or nonsurgical, you'll go through a rehabilitation program involving physical therapy exercises to strengthen your leg muscles and Achilles tendon. Most people return to their former level of activity within four to six months.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.Causes
The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture.
Symptoms
Following are a few of the symptoms usually associated with an Achilles tendon rupture. Sudden, severe pain, swelling, bruising, difficulty walking. Sometimes a gap may be felt in the tendon. The most common ways an Achilles tendon rupture is diagnosed are clinical history (presenting symptoms). Thompson or Simmonds test, positive if when squeezing the calf there is no foot movement (passive planter flextion). OBriens test, needles are placed into the tendon; tendon is intact if when the foot is moved up and down, the needle hub moves in the same direction as the toes (opposite direction of the tendon) Ultrasound and MRI, because these technologies involve an added expense, they are usually employed only to confirm the diagnosis.
Diagnosis
A typical history as detailed above together with positive clinical examination usually will clinch the diagnosis. In an acute rupture, one can usually feel the gap in the tendon from the rupture. There may be swelling or bruising around the ankle and foot of the injured leg. With the patient lying on the tummy (prone position) with the knee flexed, the examiner should see the ankle and foot flex downwards (plantarward) when squeezing the calf muscles. If there is no movement in the ankle and foot on squeezing the calf muscle, this implies that the calf muscle is no longer attached to the heel bone due to a complete Achilles tendon rupture.
Non Surgical Treatment
The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex, Advil, Motrin, Naprosyn. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.
Surgical Treatment
Surgery is a common treatment for a complete rupture of the Achilles tendon. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons. Surgical complications can include infection and nerve damage. Infection rates are reduced in surgeries that employ smaller incisions. After treatment, whether surgical or nonsurgical, you'll go through a rehabilitation program involving physical therapy exercises to strengthen your leg muscles and Achilles tendon. Most people return to their former level of activity within four to six months.
 RSS Feed
RSS Feed